
Testosterone and Estrogen Levels in Women
A Measurement Question

It’s important to understand that comparing testosterone and estrogen levels in women isn’t just a simple black and white issue, it is actually far more nuanced than that. I think I need to get into the details of this because it’s important to both our understanding of how hormones are measured and how we look at the overall picture.
This is the crux: Whether testosterone is higher than estrogen in women really depends on what you are actually measuring and when.
I do think it is worth pointing out that the data referenced in our article and in this substack comes from peer-reviewed research that has been examined, challenged, and tested by experts before publication. Peer review does not make something perfect, but it does mean the data has been scrutinized and the conclusions have been held to a standard. There is a big difference between saying something on social media and publishing it in a peer-reviewed journal.
Also, our paper addresses testosterone’s physiologic role across the female lifespan and isn’t a simple head-to-head comparison of blood levels. And even if it were, the science is not as straightforward as saying one number is higher than another and calling it a day. Testosterone and estrogen are not measured the same way, they don’t behave the same way in the body, and circulating blood levels are only a piece of a much more complex picture.
First, a little history
For many years when researchers measured testosterone levels in women’s blood they used tests called immunoassays. The problem with this type of testing is that the results were picking up the wrong thing. They were supposed to measure testosterone, but they were also including other hormones floating around in the blood - particularly DHEA, made by the adrenal glands. So the testosterone readings looked much higher than they actually were. It took us a while to figure that out and correct it (Stanczyk FZ, Vesper H. Menopause 2025).
Modern testing - called liquid chromatography tandem mass spectrometry, or LC-MS/MS - fixed this. It measures testosterone specifically without picking up everything else. This matters a lot for understanding what the research actually shows.
What the blood tells us
With modern testing, circulating estradiol (the most biologically active estrogen) is higher than testosterone in the bloodstream of premenopausal women. Research from Skiba and colleagues using LC-MS/MS in a large cohort of women confirmed this clearly (Skiba MA et al. J Clin Endocrinol Metab 2019). And when you add in all the other estrogens women produce - estrone and estriol - total circulating estrogens are substantially higher than testosterone in premenopausal women.
So if someone tells you circulating estrogen is higher than testosterone in premenopausal women they are correct. That is what the blood shows with modern testing. But what is circulating in the blood is only one part of the story. What the body produces, converts, and uses throughout the day is another.
Both of these statements are true. We just keep measuring what is in the blood at a moment in time and calling that the whole story, and of course it is not.
The blood level is just a snapshot
We all know that a blood test only shows you what is circulating at one moment in time, which is why we don’t recommend hormone testing in perimenopause. Your body is constantly producing hormones, converting them into other hormones, using them in tissues throughout the body. What shows up in a blood draw is just a small part of what is actually happening.
When researchers measured daily hormone production rates using a completely different methodology called isotope dilution studies, which were not affected by the old immunoassay problems, they found that daily testosterone production in reproductive-aged women exceeds estradiol production. Estimates vary depending on the method used to measure it, and that variation is a perfect example of the larger point - how you measure hormones shapes what the result is (Burger HG et al. Recent Prog Horm Res 2002).
That production estimate is also likely conservative. It does not fully account for all the androgen precursors - hormones like DHEA and androstenedione - that are constantly being converted into testosterone in your tissues, your fat cells, your muscles, and your brain throughout the day (Goldman AL et al. Endocr Rev 2017).
The same logic applies to both sides
When researchers argue that total estrogens are higher than testosterone - by including estrone and estriol alongside estradiol - they are making a valid point. But the same logic can apply to testosterone.
Testosterone has its own family of precursor hormones that convert into testosterone throughout the body. Just like total estrogens exceed estradiol alone in the blood, total androgens significantly exceed what you see as testosterone in a single blood test. Both hormone families are being underrepresented by any one measurement (Goldman AL et al. Endocr Rev 2017).
We all know that the way we measure testosterone and estradiol are with different units. Testosterone operates at nanomolar concentrations in women compared to the picomolar concentrations of estradiol (Davis SR, Wahlin-Jacobsen S. Lancet Diabetes Endocrinol 2015). A nanomole is a thousand times larger than a picomole. These are very different orders of magnitude - both documented in the peer reviewed literature - and they help us understand hormone activity in the body.
What the data looks like over a lifetime
The figure below from Mauvais-Jarvis and Lindsey published in the Journal of Clinical Investigation in 2024 shows circulating testosterone and estradiol in males and females across the entire lifespan - measured in the same units using gold standard LC-MS/MS testing on CDC NHANES data from over 14,000 people.
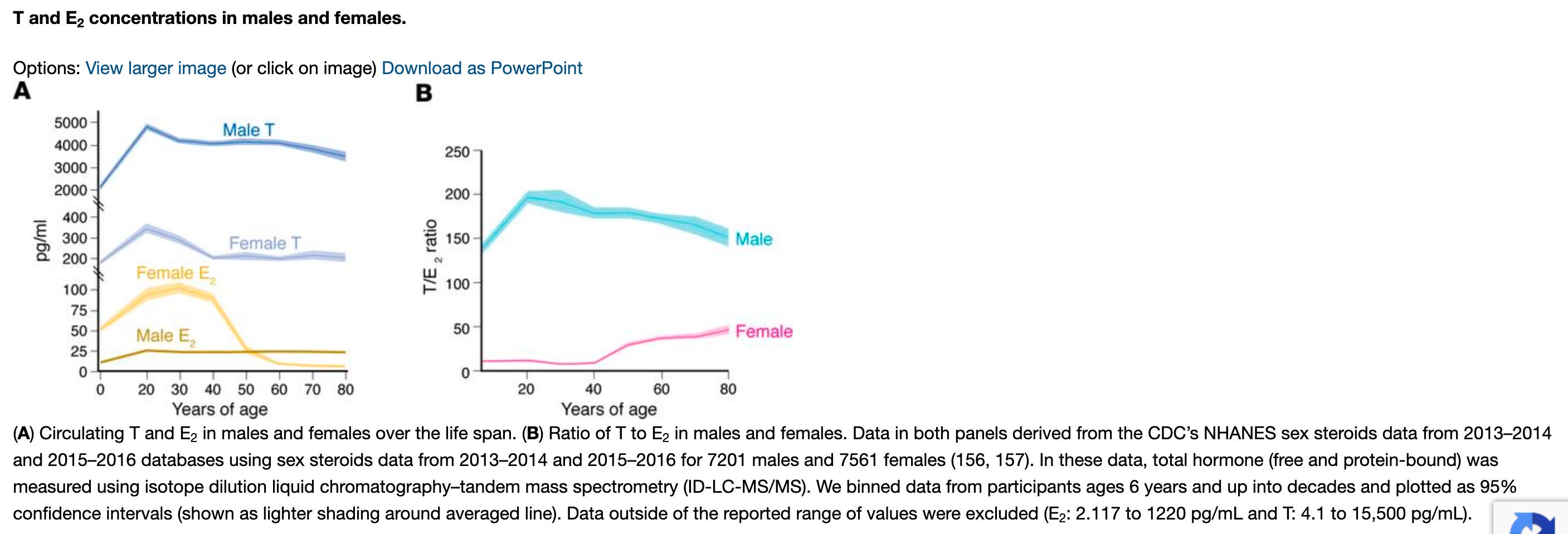
Figure 2 from Mauvais-Jarvis F, Lindsey SH. J Clin Invest. 2024;134(17):e180073. Panel A shows concentrations in pg/mL across the lifespan. Panel B shows the ratio of testosterone to estradiol across the lifespan in both sexes.
A few important points about these graphs. First - both hormones are measured in the same units using the same (gold standard) methodology. This is not an apples to oranges comparison. Second, this figure compares testosterone to estradiol alone, not total estrogens. When you include estrone and estriol, total circulating estrogens exceed testosterone in premenopausal women, consistent with the Skiba data. Third, Panel B shows the testosterone to estradiol ratio across the lifespan. Even in women that ratio is consistently above zero, meaning testosterone is always present and measurable.
The authors state directly in the Mauvais-Jarvis article that testosterone is the most abundant circulating active sex steroid in females across the lifespan and may circulate at concentrations roughly 5–50 times higher than estradiol depending on the life stage being evaluated. That range makes sense when you think about it - estradiol drops dramatically after menopause while testosterone declines more gradually, so which hormone appears higher really depends on which women you are measuring and when.
So what is actually true?
I think we can say that all of this is true.
Circulating estrogens are higher than testosterone in the bloodstream of premenopausal women when you use the right testing (Skiba MA et al. J Clin Endocrinol Metab 2019).
Daily testosterone production significantly exceeds estradiol production in reproductive aged women - though how much depends on how you measure it (Burger HG et al. Recent Prog Horm Res 2002).
The total amount of androgens (not just testosterone) in your blood is much higher than what shows up on a testosterone blood test - just like total estrogens are larger than estradiol alone. Also true (Goldman AL et al. Endocr Rev 2017).
And over the female lifespan, including post-menopause, testosterone is the most abundant circulating active sex steroid, running 5 to 50 times higher than estradiol (Mauvais-Jarvis F, Lindsey SH. J Clin Invest 2024).
None of these findings contradict each other; they are just answering different questions.
What really matters
Here is what we should actually be focusing on: in a recent analysis of over 33,000 women aged 18 to 70 years diagnosed with hypoactive sexual desire disorder only 850 were ever prescribed testosterone, which is less than 3 percent (Agrawal P et al. J Sex Med 2024). Even accounting for prescriptions not captured in that data, that gap is just not acceptable.
Part of what drives that gap is confusion about what testosterone is, what it does, and what the research actually shows. We need to give our patients more than just a conclusion, so women don’t lose the ability to have informed conversations with their clinicians and miss out on treatment.
The bottom line
The next time you see testosterone and estrogen described in absolute terms - one higher, one lower, case closed - ask what is actually being measured. Blood levels or production rates? Estradiol alone or total estrogens? Testosterone alone or the full androgen pool?
The answer to each of those questions is different and all of them are correct. We just have to be very careful to understand that things aren’t always black and white.
References
Agrawal P, Singh SM, Hsueh J, et al. Testosterone therapy in females is not associated with increased cardiovascular or breast cancer risk: a claims database analysis. J Sex Med 2024;21:414–9.
Burger HG, Dudley EC, Robertson DM, et al. Hormonal changes in the menopause transition. Recent Prog Horm Res 2002;57:257–75.
Davis SR, Wahlin-Jacobsen S. Testosterone in women — the clinical significance. Lancet Diabetes Endocrinol 2015;3(12):980–92.
Goldman AL, Bhasin S, Wu FCW, et al. A reappraisal of testosterone’s binding in circulation: physiological and clinical implications. Endocr Rev 2017;38(4):302–24.
Lanoff J, Simon JA. Testosterone in women: clinical evidence and practice guidelines. Obstet Gynecol Clin N Am 2026. https://doi.org/10.1016/j.ogc.2026.03.003
Mauvais-Jarvis F, Lindsey SH. Metabolic benefits afforded by estradiol and testosterone in both sexes: clinical considerations. J Clin Invest 2024;134(17):e180073.
Skiba MA, Bell RJ, Islam RM, et al. Androgens during the reproductive years: what is normal for women? J Clin Endocrinol Metab 2019;104(11):5382–92.
Stanczyk FZ, Vesper H. Challenges in developing accurate assays for the measurement of estradiol and testosterone in postmenopausal women. Menopause 2025;32(12):1149–56.